

Is Movement the missing piece for you?
Is Movement the missing piece for you?
If you haven't had your movement assessed well, then read on!

Why Movement?
It is my belief that there are principles that offer you the best chance to make progress with painful symptoms. Movement and the exploration of movement is one of those principles.
Your current movement strategies are the best available options that your nervous system can utilise at any given time. These “available options” are the subject of today's Substack.
We have 360 joints & 639 muscles that control and produce movement in the human body. Almost every joint in the body has movement in 3 planes of motion as described in the diagram below.
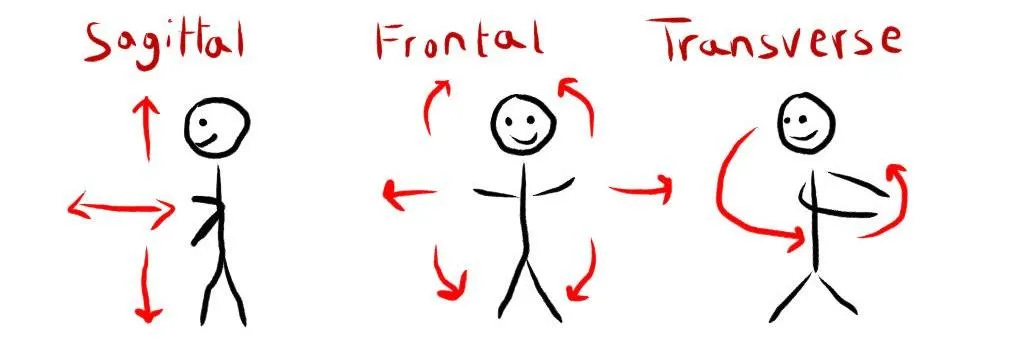
Sagittal: up and down movement - think bending forwards and then standing up straight again.
Frontal: side to side movement - think sliding your hand down the outside of the thigh and then returning to standing straight.
Transverse: rotational movement - think turning your head from side to side or turning your forearm from palm facing the sky to palm facing the floor
So far we have 360 joints and almost every joint will experience movement in each of these 3 planes of motion. 1050+ possible joint motions 😳 - but that’s not all….
Walking Gait - the Human Movement Framework
If we assess this all during walking, there are (depending on how you look at it) 6-7 major phases of walking gait where every joint in your body should experience movement in all available planes of motion.
This doesn't mean each joint will move through it's full range of movement - that would make for some strange walking patterns!
360 joints X 7 phases of movement X 3 planes of motion = ~7560 available joint motions that ideally could happen with every footstep.
Mind-blowing.
This makes me think of the classic scene in the Matrix when Neo sees the matrix for the first time! Human movement is amazing and complex.

However we can make it more simple and useful for a person in pain. So, how do we do this?
If we know that there are thousands of combinations of joint motions that could be available, it must be important to understand when those joint motions are supposed to happen.
If we have at least got a framework to work from - it should be possible to assess a person's movement as accurately as possible and figure out what movements their body struggles with. In my membership community and course site, I have built a process for my clients to assess their own movement and gain insight into the areas of their body that are struggling to move well.
It's pretty logical; if we can find out where your body is struggling to move well & we have a framework that helps us to understand when that movement should ideally occur - we can then work to close the gap between both and restore what's missing.
A big part of rehab that I believe gets missed is positive transfer.
Positive transfer in movement refers to the facilitation, in learning or performance, of new movement based on what has been learned during a previous one.
Does the exercise that you are doing transfer across to habitual movement change?
If it doesn't, you are getting stronger (not a bad thing) and also might fail to change a loading strategy because the exercise hasn’t facilitated a change in your movement patterns.
We must also consider that bodies are very clever and often can very successfully avoid moving or loading certain structures by shifting where the load goes through subtle movement alterations.
How might movement compensation occur?
At every joint, there is what we call a physiological range of movement. Aka a normal range of degrees that the joint should be able to move through.
For ease of understanding, let's say there are 20° of movement possible at my joint. Perhaps I have injured or sensitised some tissues from 11-20° of the joints range. My clever nervous system may still be able to complete my sport or movement task by sharing load from 1-10° at that joint and asking the next tissues or joints to take up the extra loading that I didn't access.
These degrees of freedom are important. For me, they mean that our incredibly adaptable bodies can keep us moving and going really really well in the vast majority of cases. It may be in a compensated way but still gets us from A to B.
Where this seems to change is when injury, structural changes, tissue sensitivity or perhaps learned behaviour change starts to greatly restrict some of these degrees of freedom.
Imaging the same joint, but now, only 17-20° of movement are possible. 1-16° are deemed unsafe and aren't available for sharing load. Now we have 3° available at the joint in question.
It should be fairly obvious to understand that every tissue that is subjected to load during those 3° of movement are likely to take a lot more loading than if there were 20º available. That is not likely to be the happiest set of tissues or joint movements in a human body.
Why does this matter?
In my clinic I will often meet people who feel tight, stiff and sore. Many of these people are getting soft tissue treatments, foam rolling and stretching or mobilising as much as they can and are still feeling tight, stiff and sore.
Despite their best efforts, they are still not getting the changes they want. Often this is because the body part that can't move well is never identified.
Your sore lower back that never seems to fully resolve might be because your neck doesn't want to side bend and lacking the ability to side-bend your neck means that your spine and lower back always adopt the same postures and load the same tissues.
Sometimes the cascade of compensatory changes creates the symptom - aka - the symptoms are created by the body's solution, not the problem.
Take the solution away, you increase or expose a problem area. Increase that exposure and you require a bigger more forceful solution. This snapback or rubberband effect is common and clients will often become infuriated by previous attempts to overcome symptoms only for them to return time and time again. Sound familiar?
Circling back around to movement again - if you have only ever been assessed on a treatment table and only the painful body parts have been poked, prodded and treated, how much insight have you and your therapist gained about your problem?
The sore hip, sore big toe and sore shoulder all have one thing in common. They are supposed to move and contribute to a movement ecosystem. Just like in an ecosystem, if you mess with one part you have a ripple effect throughout the rest.
Appreciating the movement strategy your body currently uses and mapping that out in relation to previous injuries and current symptoms will often paint a picture that is simpler than you expect:
Get that spine able to sidebend and rotate again after its movement has been affected by a previous whiplash
Get that hip to experience a quality hip extension again after that approx removal that happened about 6 months prior to the hip pain beginning.
Pronate and supinate those feet after multiple ankle sprains to alleviate that pesky knee symptom that shows up when you run.
Etc etc etc.
Not considering movement is like being tasked with building a skyscraper but all you have is wattle and daub. You are going to be able to do something, but it's unlikely to be very effective or get above the first floor!
Finding some help…
If you haven't yet worked with someone who looks at how your whole body moves in an interconnected way, consider doing a little bit of research to find a movement professional in your area.
The link below contains a database of movement practitioners that have trained in some of the same schools of thought as I have. I cannot guarantee their quality, only that they have been exposed to and likely use this type of approach.
Find a movement practitioner here.
If you cannot find anyone near you on that list and you fancy working in an online capacity, you can get access to my membership site and make an appointment with me by clicking this link:
http://move-out-of-pain.mn.co
As always, if you have enjoyed this and feel like someone you know would like to read it, please share it with them.
Move well,
David